ACO Lifts HCC Capture by 34% in One MA Plan Year
Year-2 reconciliation for Summit Health Alliance ACO revealed $4.6M in lost risk-adjusted revenue. The CFO made it clear to the board that this outcome would not repeat — but he needed a concrete operational mechanism to ensure it.
Business Challenges
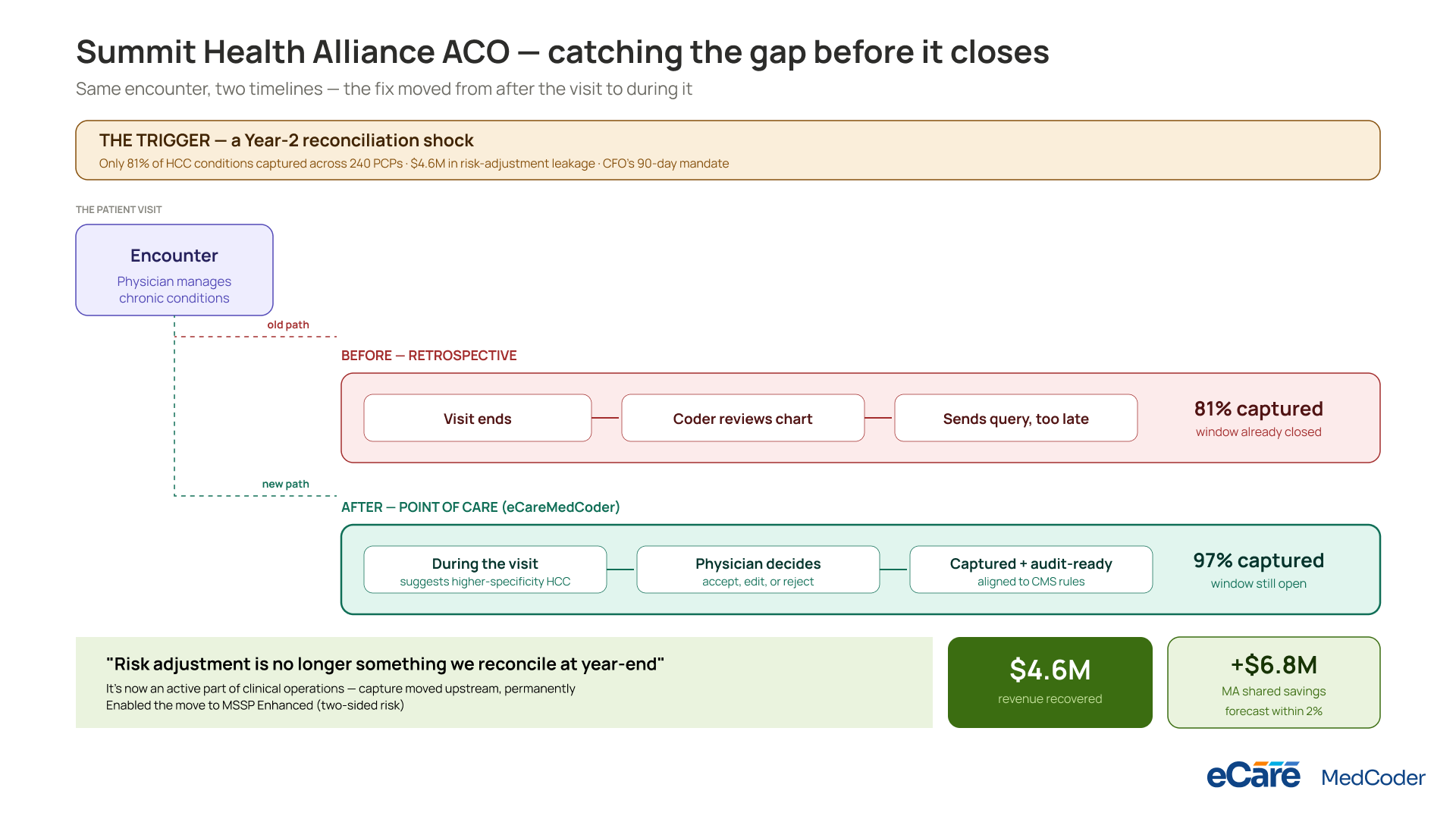
In October 2025, Summit Health Alliance received its Year-2 reconciliation report under its value-based care contract. The results exposed a significant shortfall. Across 240 primary care physicians managing nearly 88,000 attributed members in the Mountain West, the organization had only captured 81% of expected HCC conditions. The remaining gap translated into roughly $4.6M in missed risk-adjustment payments.
For CFO Eli Markowitz, the issue was not just financial — it signaled a systemic weakness in documentation practices. Clinical care delivery was not the problem; physicians were actively managing chronic conditions, but the supporting documentation lacked the specificity required for risk adjustment. Conditions were often recorded in broad categories rather than coded with the level of detail needed for HCC attribution, even when clinical evidence supported it.
The ACO’s coding process relied heavily on retrospective chart review. Coders reviewed encounters after the fact, submitted clarification queries, and attempted to correct gaps post-visit. While effective to a degree, this approach introduced delays and left many documentation gaps permanently uncorrected due to timing and billing constraints. Eli concluded that the issue had to be addressed at the point of care rather than downstream.
- HCC capture stood at 81% of expected levels
- Estimated $4.6M in risk-adjustment leakage
- Under-specific clinical documentation across chronic conditions
- Retrospective coding limited correction opportunities
- Significant variation in documentation quality across physicians
Solution
Eli mandated a 90-day implementation requirement aligned to the ongoing performance year. The goal was to embed documentation improvement directly into clinical workflows before encounters were finalized.
The selected platform, eCareMedCoder, introduced real-time documentation support during patient visits. Instead of replacing physician input, it analyzed clinical context and suggested higher-specificity HCC conditions at the point of care. Physicians could accept, edit, or reject recommendations, maintaining clinical autonomy while improving coding precision.
A key differentiator was audit readiness. Every captured condition was structured to align with CMS audit requirements, reducing exposure to retrospective recoupment. This was particularly important for the CFO, who needed improved capture without introducing compliance risk.
Value Delivered
By the end of Year 3, HCC capture rose to 97% of expected benchmarks, reversing the prior year’s leakage and restoring approximately $4.6M in risk-adjusted revenue.
- HCC capture increased from 81% to 97%
- Full recovery of $4.6M previously missed revenue
- Shift from retrospective coding to point-of-care capture
- Standardized documentation quality across all 240 PCPs
- Forecast accuracy improved to within 2% variance
Solution Provided
The rollout took place over 16 weeks and prioritized high-impact practices to accelerate financial recovery while scaling system-wide consistency.
Weeks 1–4: Top 8 Practices (Highest HCC Leverage)
The initial phase focused on eight practices accounting for nearly 40% of attributed members. These groups offered the highest immediate financial return, so deployment concentrated on integrating real-time documentation support into live patient encounters.
Weeks 5–9: Practices 9–22
The next group included 14 practices. By this stage, implementation workflows were stabilized, allowing practice managers to incorporate weekly HCC performance monitoring into their regular operational reviews.
Weeks 10–13: Practices 23–31
The final set of nine practices joined the system. Although individually smaller, their inclusion ensured consistency in documentation standards across the entire network.
Weeks 13–16: Network-Wide HCC Capture Monitoring and Quality Loop
A centralized reporting system was established for ongoing oversight. Eli received weekly updates on HCC performance by practice, with targeted intervention deployed where gaps persisted. This created a continuous feedback loop rather than a one-time correction effort.
Business Value
Eli presented the Year-3 outcomes to the board in October 2026, a year after the initial financial gap was identified. The focus shifted from remediation to operational maturity.
What changed about the ACO’s risk-adjustment posture
HCC capture became a continuous, embedded process rather than a year-end reconciliation issue. Financial forecasting improved significantly, with variance reduced to within 2% of actual results.
The financial picture
The ACO recovered $4.6M in previously lost revenue, with sustained annual value estimated at around $5M going forward. The implementation cost was $720K, generating a strong return within the first year.
What changed about ACO governance
Improved performance strengthened the ACO’s standing in value-based contracts, enabling transition to MSSP Enhanced (two-sided risk), reflecting increased confidence in risk management capabilities.
“Year 2 highlighted the gap in our system. Year 3 showed it could be fixed structurally. Risk adjustment is no longer something we reconcile at year-end — it is now an active part of clinical operations. That shift is what ensures this problem doesn’t return.” — Eli Markowitz, CFO, Summit Health Alliance ACO

